GMHC’s National Webinar on HIV and Aging featured encouraging news about next-generation HIV therapies and strong support for moving past a biomedical treatment emphasis to a more holistic care model for people over age 50 living with HIV.
National AIDS Policy Director Harold Phillips said in his keynote speech that he aims to unveil the Biden administration’s new national HIV/AIDS strategy by World AIDS Day on Dec. 1. Phillips, himself over 50 and living with HIV, said he wants to “ensure an adequate federal response to those living and aging with HIV,” that supports a broader-based, wraparound care model.
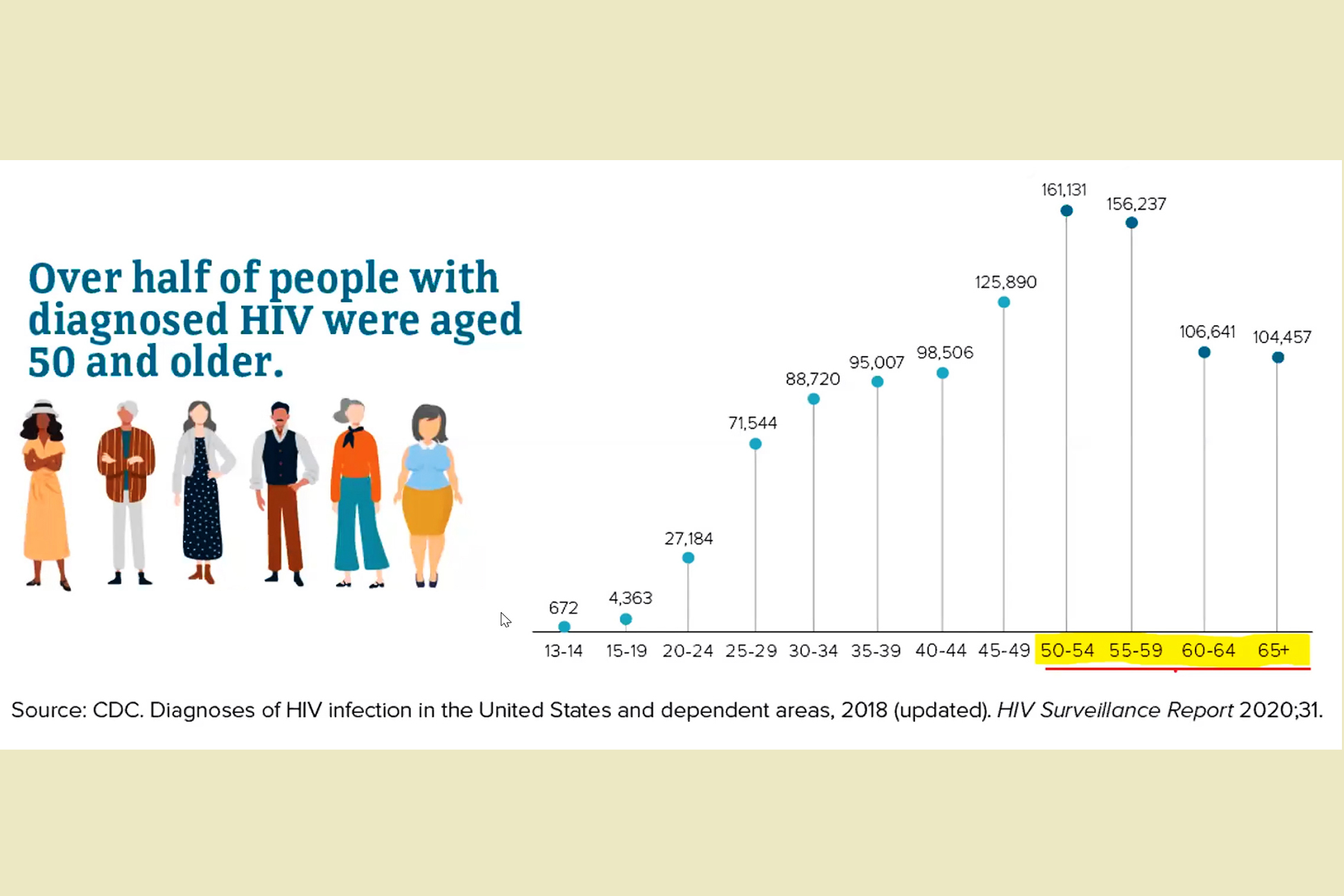
That’s essential, said the HIV researchers, patient advocates, and activists who spoke at the national webinar on Sept. 14, since an estimated 70% of people living with HIV will be age 50 or older by 2030.
“Managing viral loads is the backbone of care,” said Stephen Karpiak, the director of GMHC’s National Resource Center on HIV and Aging and the webinar’s organizer, but he added that new care models are urgently needed to address co-morbidities for people aging with HIV.
This population experiences higher risks and, often, an earlier onset for diseases associated with aging—such as heart, kidney and bone diseases, diabetes, cancers, arthritis, and cognitive impairment—at rates two to five times higher than that of HIV-negative people of similar age.
“Older people aging with HIV/AIDS must be heard,” Karpiak emphasized.
Phillips said HIV testing and treatment for older adults must be more proactive. An estimated 18,800 people over age 50 with HIV are undiagnosed, he said, and when diagnosed, older adults are more likely to have late-stage HIV infection.
People ages 50 and over accounted for one in six of new HIV diagnoses in 2018, he added. Men made up the majority with 3,019 cases, of which 66% were for men who have sex with men. But 1,815 of the new diagnoses were for women over 50, with 86% from heterosexual contact and 14% from IV drug use.
“We’ve still got work to do,” Phillips said. Older adults “may need help in disclosing an HIV diagnosis to family and friends,” he added, which is important to prevent isolation, and gain care and support.
There’s a need for better medical care and wraparound support to overcome treatment barriers, Phillips said, to ensure older adults living with HIV have adequate food, housing, transport, and mental and behavioral health supports.
Phillips said his office is assessing how to modernize the federal Ryan White HIV/AIDS Program to ensure it addresses the needs of people ages 50 and older, who already make up more than half of people living with HIV in the US. Another focus is assessing the National Institutes of Health’s research priorities to place more emphasis on HIV co-morbidities, in addition to reducing the incidence of HIV, next-generation HIV treatment therapies, and a cure.
The major issue addressed by the advocates and activists participating in the webinar—many of whom are living with HIV themselves—was that older adults living with HIV are often excluded from the conversation around improving their care.
“We want the healthcare system to recognize that you have to treat the whole person, which incorporates physical, mental and spiritual health, for people who are aging with HIV—and, often, living alone in isolation,” said Melanie Reese, the executive director of Older Women Embracing Life, which serves women living with HIV in Baltimore and Washington, D.C.
“Yes, we are living longer, but we want to have a robust quality of life,” Reese said. “We have to advocate for whole-person care, and take that agenda to the streets—to your local, state and federal government.”
Next-Gen HIV Meds
There is good news as far as treatment, said Mark Milano, the Lead Trainer for ACRIA Centers at GMHC. Longer-acting HIV-prevention and treatment medications to be taken monthly, not daily, are already available—and others are in the works to be taken just every six months.
The FDA approved the first injectable, monthly HIV medication, cabenuva, in January. Right now, the antiretroviral medication is administered once per month in two shots (one of cabotegravir and one of rilpivirine), but that will likely change to every other month by next year, Milano said.
Another new drug in the pipeline is islatravir, which could possibly be used for both PrEP (pre-exposure prophylaxis) and PEP (post-exposure prophylaxis) as a monthly pill, or even as an annual implant for PrEP. That’s still in clinical trials and a year or two away, Milano said.
One medication that could be a “game-changer,” he said, is lenacapavir, an experimental capsid inhibitor, which could work at more than one point in the HIV lifecycle. Unlike antiretrovirals, which block the enzyme that an HIV-infected cell uses to replicate its RNA, capsid inhibitors act on the capsid, the name for the proteins surrounding HIV’s genetic material.
Lenacapavir is being tested for injection once every six months, Milano said, with a 94% reported efficacy rate for first-time HIV-medication takers and 81% efficacy for those who are multi-HIV-drug resistant.